Oct 07, 2023
SUMMARY
Abstract
Several models of the progress of dementia in the UK change suggests a 57% increase in the number of people with dementia from 2016 to 2040, 70% of that expected If age-specific incidence rates remained steady, such that by 2040 there will be 1.2 million UK citizen with dementia. Models also suggest that there will be future increases in number of individuals with dementia and Alzheimer's which is considered as a type of dementia.
NTRODUCTION
The population increase in geriatrics in the recent years draws attention. It is known that there are approximately 57.4 million dementia patients in the world in 2019, and this number is estimated to tripled by 152.8 million in 2050. Research leads are now focusing on finding ways to prevent dementia. Although age is an important risk factor in dementia it can't be considered as the exact reason. As nutrigenetic - epigenetic mechanisms begin to be understood, a small part of genetic predispositions become effetive, but it is possible to reduce epigenetic negativities and reduce dementia development by predetermining genetic dementia, depression, high blood pressure, high cholesterol, vitamin need and predisposition to inflammation and applying a suitable lifestyle, nutrition and sports.
Overall, a growing body of evidence supports the nine potentially modifiable risk factors for dementia modelled by the 2017 Lancet Commission on dementia prevention, intervention, and care:
less education,
hypertension,
hearing impairment,
smoking,
obesity,
depression,
physical inactivity,
diabetes,and
• low social contact .
Age, family history, heart disease, diabetes, stroke, high blood pressure, high cholesterol, the presence of a genetic variant in one or two Apoprotein E (APOE) or other dementia susceptibility or the detection of genes that protect from dementia are important in early ages.
TECHNICAL SUMMARY
On the technical side it is important to determine the genetic differences of proinflammatory cytokines such as tumor necrosis factor-α, interleukin 1 beta (IL-1β) and interleukin 6 (IL-6) in Dementia where inflammation plays and improtant role. Variants of some genes can also be evaluated to protect against Alzheimer's disease.
Since the susceptiblity to demetia is important in HTR2A and depression-prone people in the relationship between serotonin and Alzheimer's, variants of the TPH2 gene have been associated with Alzheimer's, variants of the TPH2 gene have been associated. Some genes variants have also been associate with Alzheimer's.
FOUR P’S
This is the basis for personalised medicine and by understanding the role our DNA plays in our health, it can help us transform how we think about our healthcare and help us deliver the Four Ps.
Four Ps:
Prediction and Prevention of disease
Precise diagnosis
Personalised and targeted interventions
Participatory role for patients
Therefore, the importance of genetic testing in detecting genetic predispositions in the prevention of dementia is increasing day by day. In addition to examining the genetic variants of increasing risk, we believe that the detection of people's predispositions to obesity, hypertension and inflammation will play an important role in the early diagnosis and treatment of dementia.
PRESICION MEDICINE AND PREVENTIVE MEDICINE
• • • • • •
Precision medicine may be helpful in assessing and reducing risk for dementia development: The idea of sequencing one’s genome to tailor their diet and lifestyle is a concept within reach. Precision medicine, a potential means of primary and/or secondary prevention, is the acquisition of the multifaceted characteristics encompassing a human being.
Clinical history,
Neurodevelopment,
Academic history,
Past and current lifestyle habits,
Environmental exposures,
Life events are analyzed.
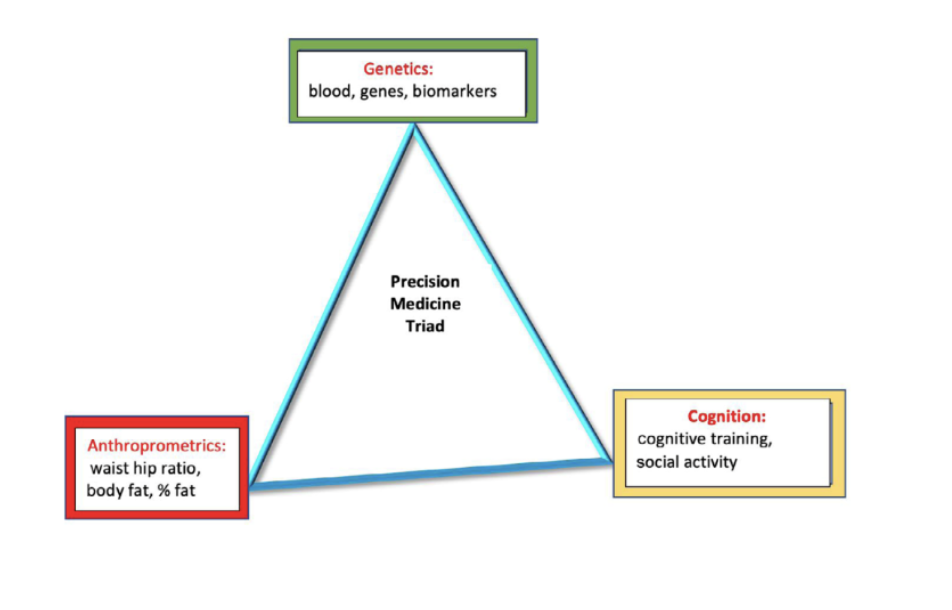
Past medical history, including physical/neurological examination are studied and then interpreted as well. Anthropometrics, the study of the proportions of the human body (body mass index, waist to hip ratio), and blood biomarkers with genetic analysis are performed. In conjunction with the physical examination, a cognitive assessment is also obtained and, along all of this invaluable information, allows us to practice “deep phenotyping”, or in other words gathering individual data about each person.
CLINICAL APPROACH
A shift of focus on risk reduction and preventative measures should also be ongoing and possibly utilized in the clinical environment. Since there is no cure for dementia, patients who are at high risk could benefit from early risk detection to possibly reduce the likelihood of developing it Given mounting evidence supporting the effectiveness of preventive measures, clinicians have an obligation to educate themselves and show their patients different options for dementia prevention.
It is the hope of these authors that this manuscript encourages more primary care clinicians to:
-Look for AD/Dementia risk factors and/or early signs of cognitive decline
-Remember that AD/Dementia risk reduction is possible, and
-Feel confident in suggesting that at-risk patients take relatively benign steps towards dementia risk reduction by emphasizing a healthy diet by the Mediterranean diet and/or MIND diet. Increasing dietary antioxidant consumption (especially Vitamin E, Vitamin C, and Turmeric) may help decrease inflammation in the brain, and alter our genome to helpsnare the process of AD/Dementia
-Non-dietary lifestyle modifications such as increased exercise and social interaction can be beneficial, may sharpen cognitive performance and improve executive function.